
5 results
Impact of measurement and feedback on chlorhexidine gluconate bathing among intensive care unit patients: A multicenter study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 13 September 2023, pp. 1375-1380
- Print publication:
- September 2023
-
- Article
- Export citation
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization – ERRATUM
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 07 October 2022, e166
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s78-s79
-
- Article
-
- You have access
- Open access
- Export citation
-
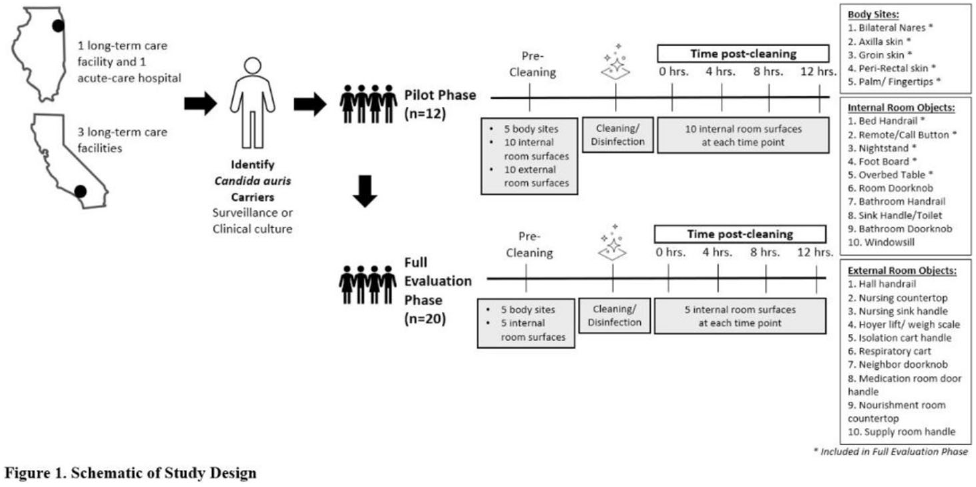
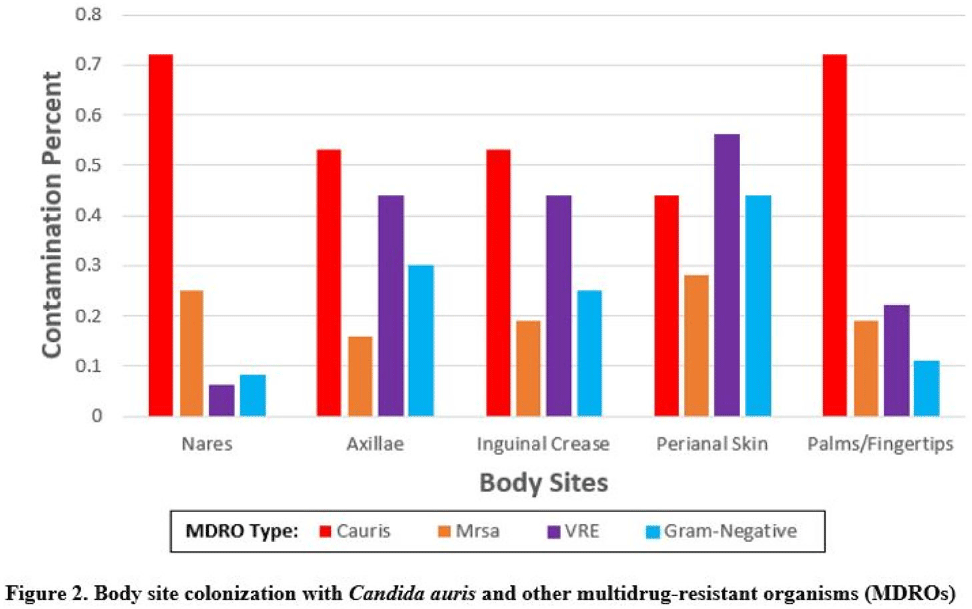
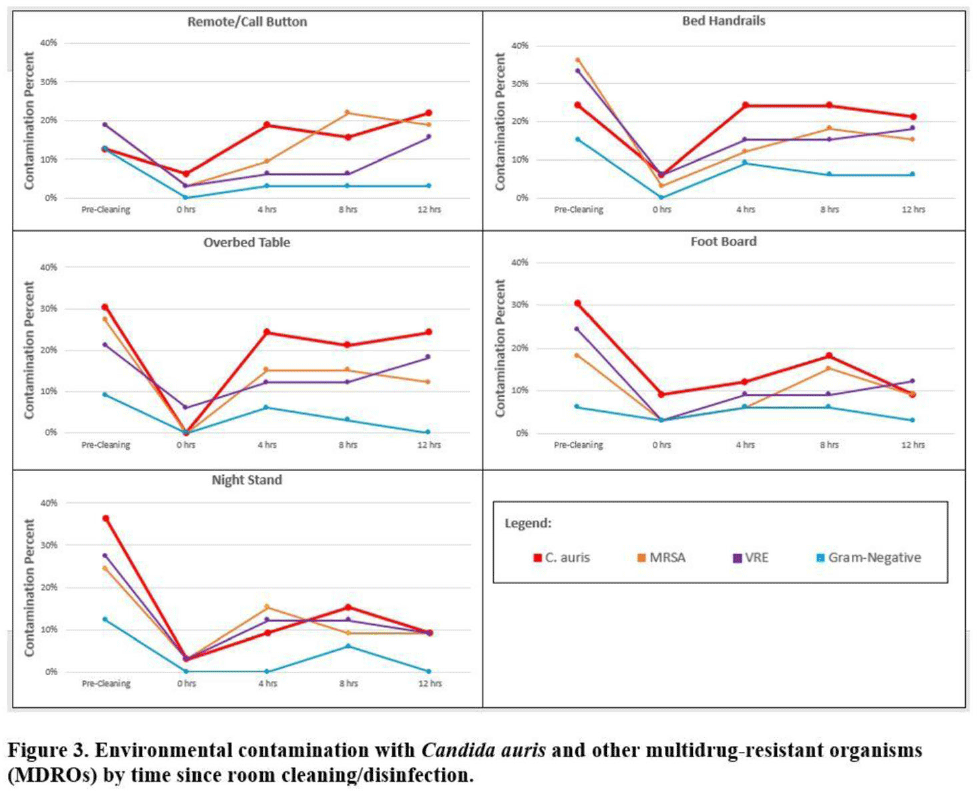
Background:Candida auris is an emerging multidrug-resistant yeast that is transmitted in healthcare facilities and is associated with substantial morbidity and mortality. Environmental contamination is suspected to play an important role in transmission but additional information is needed to inform environmental cleaning recommendations to prevent spread. Methods: We conducted a multiregional (Chicago, IL; Irvine, CA) prospective study of environmental contamination associated with C. auris colonization of patients and residents of 4 long-term care facilities and 1 acute-care hospital. Participants were identified by screening or clinical cultures. Samples were collected from participants’ body sites (eg, nares, axillae, inguinal creases, palms and fingertips, and perianal skin) and their environment before room cleaning. Daily room cleaning and disinfection by facility environmental service workers was followed by targeted cleaning of high-touch surfaces by research staff using hydrogen peroxide wipes (see EPA-approved product for C. auris, List P). Samples were collected immediately after cleaning from high-touch surfaces and repeated at 4-hour intervals up to 12 hours. A pilot phase (n = 12 patients) was conducted to identify the value of testing specific high-touch surfaces to assess environmental contamination. High-yield surfaces were included in the full evaluation phase (n = 20 patients) (Fig. 1). Samples were submitted for semiquantitative culture of C. auris and other multidrug-resistant organisms (MDROs) including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), extended-spectrum β-lactamase–producing Enterobacterales (ESBLs), and carbapenem-resistant Enterobacterales (CRE). Times to room surface contamination with C. auris and other MDROs after effective cleaning were analyzed. Results:Candida auris colonization was most frequently detected in the nares (72%) and palms and fingertips (72%). Cocolonization of body sites with other MDROs was common (Fig. 2). Surfaces located close to the patient were commonly recontaminated with C. auris by 4 hours after cleaning, including the overbed table (24%), bed handrail (24%), and TV remote or call button (19%). Environmental cocontamination was more common with resistant gram-positive organisms (MRSA and, VRE) than resistant gram-negative organisms (Fig. 3). C. auris was rarely detected on surfaces located outside a patient’s room (1 of 120 swabs; <1%). Conclusions: Environmental surfaces near C. auris–colonized patients were rapidly recontaminated after cleaning and disinfection. Cocolonization of skin and environment with other MDROs was common, with resistant gram-positive organisms predominating over gram-negative organisms on environmental surfaces. Limitations include lack of organism sequencing or typing to confirm environmental contamination was from the room resident. Rapid recontamination of environmental surfaces after manual cleaning and disinfection suggests that alternate mitigation strategies should be evaluated.
Funding: None
Disclosures: None



Indwelling medical devices and skin microorganisms on ICU patients bathed with chlorhexidine gluconate
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s43-s44
-
- Article
-
- You have access
- Open access
- Export citation
-
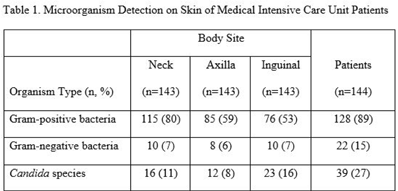
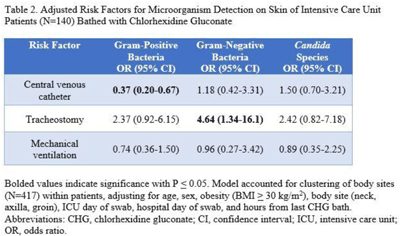
Background: Bathing ICU patients with chlorhexidine gluconate (CHG) decreases bloodstream infections and multidrug-resistant organism transmission. The efficacy of CHG bathing on skin microorganism reduction may be influenced by patient-level clinical factors. We assessed the impact of clinical factors on the recovery of microorganisms from the skin of patients admitted to an ICU who were receiving routine CHG bathing. Methods: We analyzed data obtained from 6 single-day point-prevalence surveys of adult ICU patients between January and October 2018 at 1 medical ICU, in the context of a CHG bathing quality initiative. Demographics and covariates were collected at the bedside and by chart review. Skin swabs were collected from neck, axilla, and inguinal regions and were plated to selective and nonselective media. Standard microbiologic methods were used for species identification and susceptibilities. Multivariable models included patients who received a CHG bath and accounted for clustering of body sites within patients. Results: Across all time points, 144 patients participated, yielding 429 skin swab samples. Mean age was 57 years (SD, 17); 49% were male; 44% had a central venous catheter; and 15% had a tracheostomy Also, 140 patients (97%) had >1 CHG bath prior to skin swab collection, with a median of 9 hours since their last CHG bath (IQR, 6–13 hours). Gram-positive bacteria were more commonly recovered than gram-negative or Candida spp across all skin sites (Table 1). Variation by body site was detected only for gram-positive bacteria, with recovery more common from the neck compared to axilla or groin sites. On multivariate logistic regression (Table 2), presence of central venous catheter was associated with lower odds of gram-positive bacteria recovery among those who received a CHG bath. Presence of tracheostomy was associated with a significantly higher odds of gram-negative bacteria detection on skin. No clinical factors were independently associated with recovery of Candida spp. Conclusions: Central venous catheter presence was associated with lower odds of gram-positive bacteria detection on skin, suggesting the possibility of higher quality CHG bathing among such patients. Tracheostomy presence was associated with greater odds of gram-negative bacteria detection, suggesting that it may be a potential reservoir for skin contamination or colonization. Indwelling medical devices may influence CHG bathing effectiveness in reducing microorganism burden on skin.
Funding: None
Disclosures: None


Regional Impact of a CRE Intervention Targeting High Risk Postacute Care Facilities (Chicago PROTECT)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s48-s49
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
